No dental procedure is more misunderstood than the root canal. The cultural shorthand — "I'd rather have a root canal than do that" — survives because the procedure used to be associated with significant pain, the literature on it is dense, and a small but loud strand of pseudoscience continues to claim that root canals cause cancer and chronic disease. None of that reflects the actual modern procedure, the actual peer-reviewed evidence, or the position of mainstream dentistry. Modern endodontic treatment is largely painless, supported by a century of clinical research, and one of the most successful tooth-preserving interventions available.
This guide walks you through what a root canal actually is and why teeth need them, what the procedure honestly feels like, the science vs. the myths, the real success rates from peer-reviewed long-term studies, what it costs in 2026, when retreatment or surgery makes sense after a failed root canal, and how to choose between an endodontist and a general dentist. Sources for every clinical claim are listed at the bottom — primary peer-reviewed literature, American Association of Endodontists position papers, ADA Council on Scientific Affairs statements, and Cochrane systematic reviews. Nothing here is editorial speculation; if you don't trust any specific claim, the source is one click away.
One thing worth saying up front: the goal of this post is to give you the information your dentist's chair-side conversation rarely has time for. Root canal decisions involve real tradeoffs — between saving a tooth and replacing it, between general-dentist treatment and specialist referral, between immediate relief and longer-term outcome. You deserve to make that decision with the actual facts in front of you.
What a Root Canal Actually Is
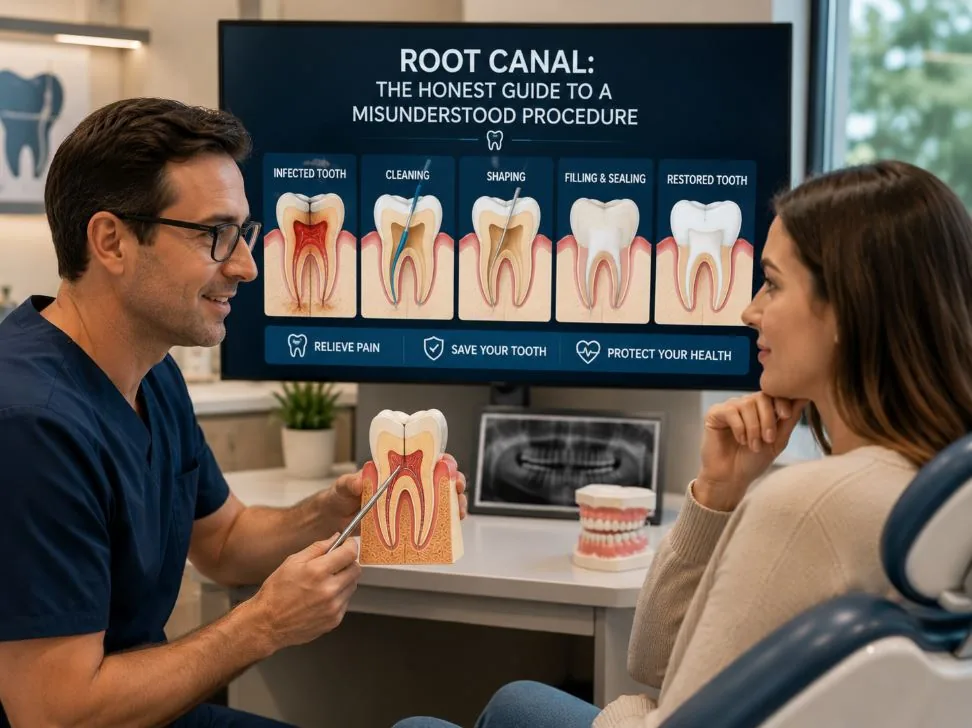
Inside every tooth is a small chamber containing soft tissue — pulp — made up of nerves, blood vessels, and connective tissue. The pulp runs from the center of the crown down through narrow channels (root canals) to the tip of each root. When that pulp becomes infected — typically because deep decay has reached it, or because trauma has disrupted its blood supply, or because a crack has opened a pathway for bacteria — the tooth has two paths forward: extract it, or treat the infection by removing the pulp, cleaning and disinfecting the canal system, and sealing the space.
The second path is what dentists call endodontic treatment — what patients usually call a "root canal." The procedure preserves the tooth's external structure (the part you chew with) by removing the source of infection inside it. Most root-canaled teeth, properly restored with a crown afterward, function for decades.
Root canal treatment is one of nine specialties recognized by the American Dental Association. The specialist is called an endodontist — a dentist who completed dental school and then a 2- to 3-year accredited endodontic residency focused exclusively on diagnosing and treating diseases of the dental pulp and periapical tissues. General dentists also perform root canals, particularly on simpler cases (single-canal anterior teeth, straightforward premolars), but endodontists handle the complex cases (curved roots, calcified canals, retreatments, surgical apicoectomies) that exceed routine general-dentistry scope.
What the Procedure Actually Looks Like
Modern root canal treatment is highly procedurally standardized. Whether your case takes one or two visits depends on the complexity and the dentist's preference, but the steps are consistent.
Total chair time for a routine single-tooth root canal is typically 60-90 minutes for a single-canal anterior tooth, and 90-120 minutes for a multi-canal molar. Two-visit cases add a 1-2 week interval between visits when the canal needs additional disinfection time before obturation.
What It Actually Feels Like
This is the question patients are most afraid to ask, and the answer is the most reassuring part of the whole procedure. The reputation of root canals as exceptionally painful is rooted in the procedure as it was performed 40-50 years ago — without microscopes, without modern rotary instrumentation, without nickel-titanium files, and often without adequate anesthesia for inflamed pulp. The procedure performed in 2026 by a competent endodontist or general dentist is fundamentally different.
Multiple peer-reviewed studies measuring intra-procedural pain on Visual Analog Scale (VAS) ratings have found that pain scores during modern endodontic treatment are statistically equivalent to or lower than pain scores during routine fillings — once adequate anesthesia is established. The American Association of Endodontists publishes patient-survey data showing the majority of patients describe the experience as no more uncomfortable than a filling.
What you'll actually experience: about 15 seconds of pinch from the anesthetic injection, a few minutes of pressure as the dentist confirms numbness, then 60-120 minutes of mild pressure sensations and the sound of instruments. Post-operative discomfort for 24-48 hours afterward is normal — typically managed with over-the-counter ibuprofen, sometimes briefly with a stronger prescription. Severe post-op pain is uncommon and usually signals a complication that should be addressed promptly.
The pain people associate with "root canals" is actually almost always the pain of the infection that led them to need a root canal in the first place. The procedure resolves that pain. By 24-48 hours after treatment, most patients report substantially less discomfort than before they walked into the office.
Endodontist or General Dentist?
Both can perform root canals legally. The decision should depend on case complexity, your dentist's experience with similar cases, and the specific anatomy of the tooth being treated.
| Best fit for general dentist | Best fit for endodontist |
|---|---|
| Single-canal anterior teeth | Multi-canal molars (especially upper second molars) |
| Straightforward premolars | Curved or calcified canals |
| Routine cases without complicating anatomy | Retreatment of previously failed root canals |
| Patients without significant medical complexity | Surgical cases (apicoectomy) |
| Cases your dentist specifically does well | Trauma cases, immature roots, special-needs sedation |
Long-term outcome studies consistently show small but measurable advantages for endodontist-treated cases on complex teeth — primarily because endodontists operate exclusively under microscopes, use specialty-tier instrumentation, and see complex cases in volume. For straightforward single-canal cases, outcomes are similar. The American Association of Endodontists maintains a public referral directory and a board-certification verification tool through the American Board of Endodontics.
How Successful Are Root Canals, Honestly?
Long-term success rates depend on the tooth, the case complexity, and the operator. Cochrane Reviews and multi-decade outcome studies in the Journal of Endodontics consistently report that initial endodontic treatment achieves long-term success in 86-98% of cases when the work is done to current standards and the tooth is properly restored afterward.
"Success" in these studies is defined rigorously — clinical absence of symptoms and radiographic evidence of healing of any periapical lesion at multi-year follow-up. The number is not "the tooth still feels okay"; it's the actual evidence-based outcome.
| Scenario | Long-term success rate (peer-reviewed) |
|---|---|
| Initial root canal, vital pulp, no periapical lesion | ~95-98% at 5-10 years |
| Initial root canal, infected pulp, no apical lesion | ~90-95% |
| Initial root canal with periapical lesion present | ~80-90% |
| Endodontic retreatment (failed prior root canal) | ~70-85% |
| Surgical apicoectomy after failed retreatment | ~75-90% |
Two factors significantly affect the numbers: quality of the coronal restoration after the root canal (a properly placed crown roughly doubles the long-term success vs. a poorly fitting temporary that leaks), and operator skill and equipment (cases done with rubber dam, microscope, and 3D imaging substantially outperform cases done without). Both factors are within your control when you choose your provider.